
Shoulder pain 3: remember the exceptions
Does teres minor muscle atrophy matter?
In the previous two posts, we introduced a case of shoulder pain in a competitive swimmer, and picked off the first of two questions we had posed ourselves, discussing some ideas regarding what might cause the teres minor atrophy seen in the report findings.
The second question, “does teres minor atrophy matter?” it turns out is actually much harder to answer.
So, does teres minor atrophy matter?
What forced us to consider this question was the pressure of a deadline. We were presenting a short talk including this case, and on the day of the talk, it occurred to one of us to ask how we would conclude our presentation. “Obviously teres minor atrophy matters and changes patient management…”, opined one of us, “…and we ought to close with a short message outlining how”. A second member of the group suggested that maybe it doesn’t matter, and what followed was a relatively animated conversation in which nobody was prepared to pick a position and stick to it.
Sparing you the entire anecdote, we have to own the fact that there was no clear answer that presented itself to us. Briefly, here are the most reasonable possibilities we ended up with.
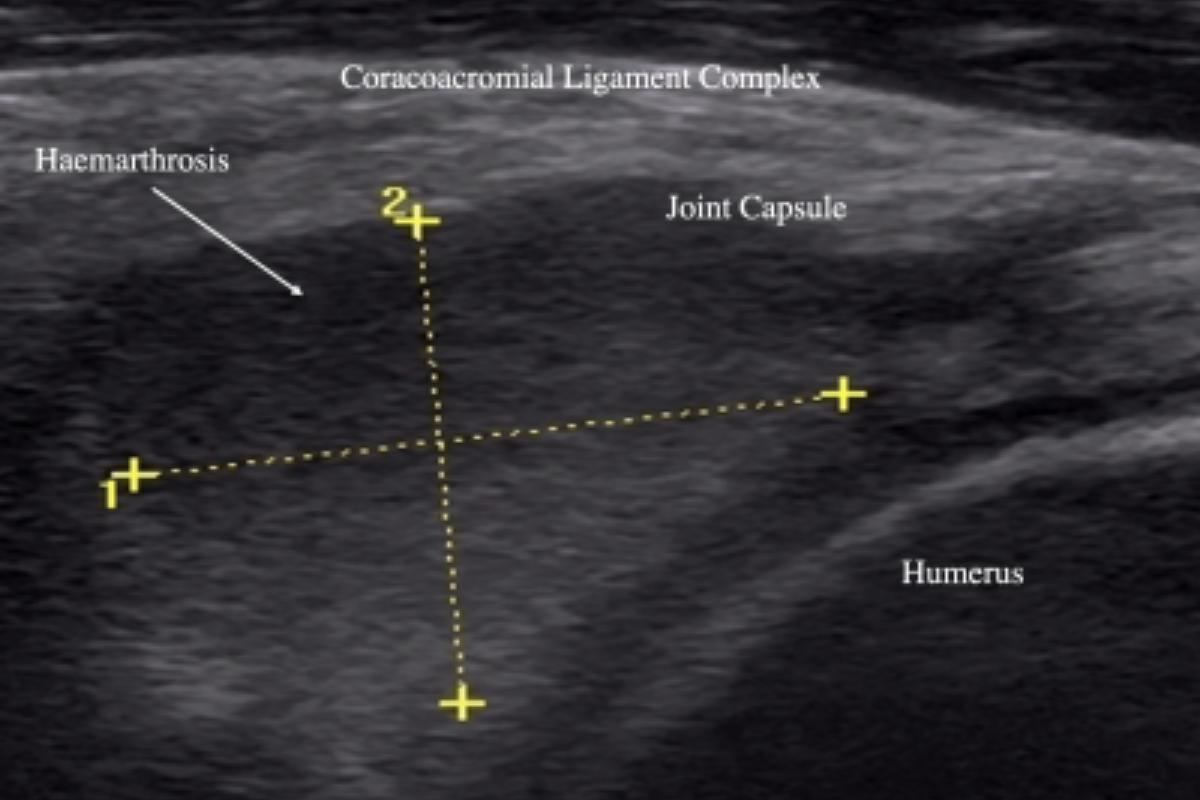
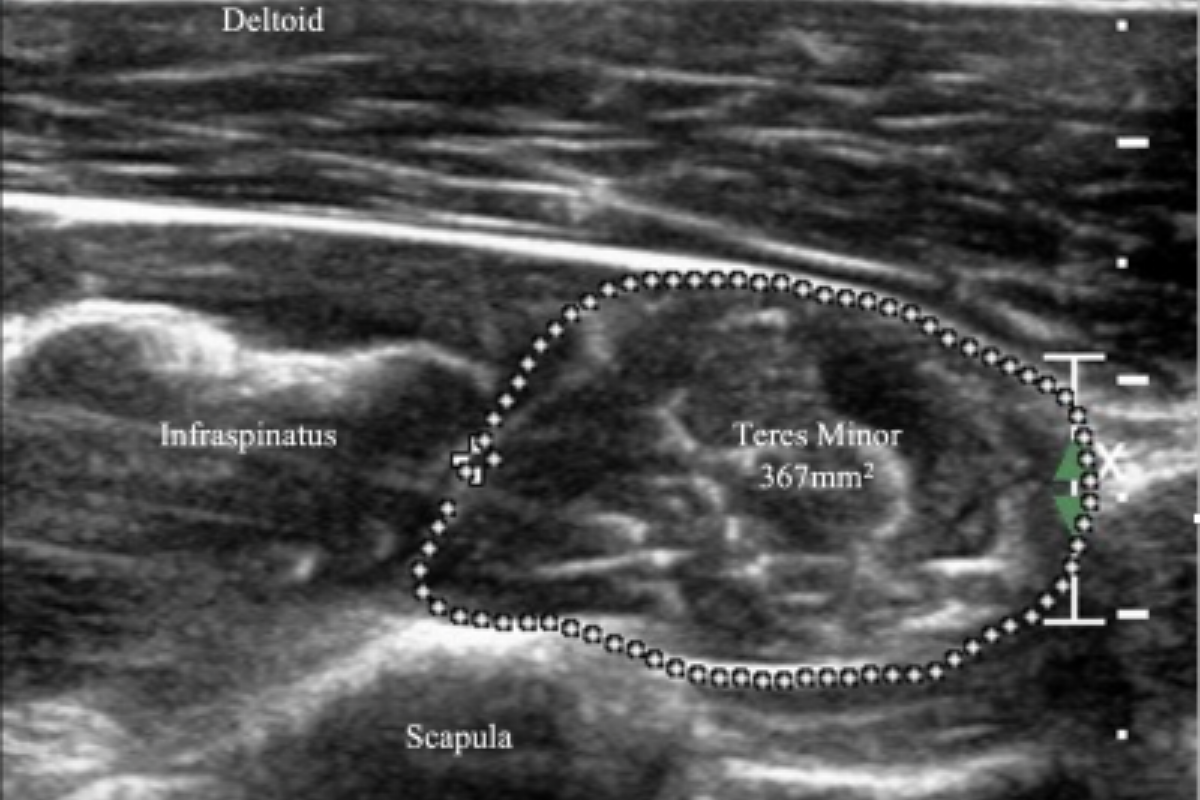
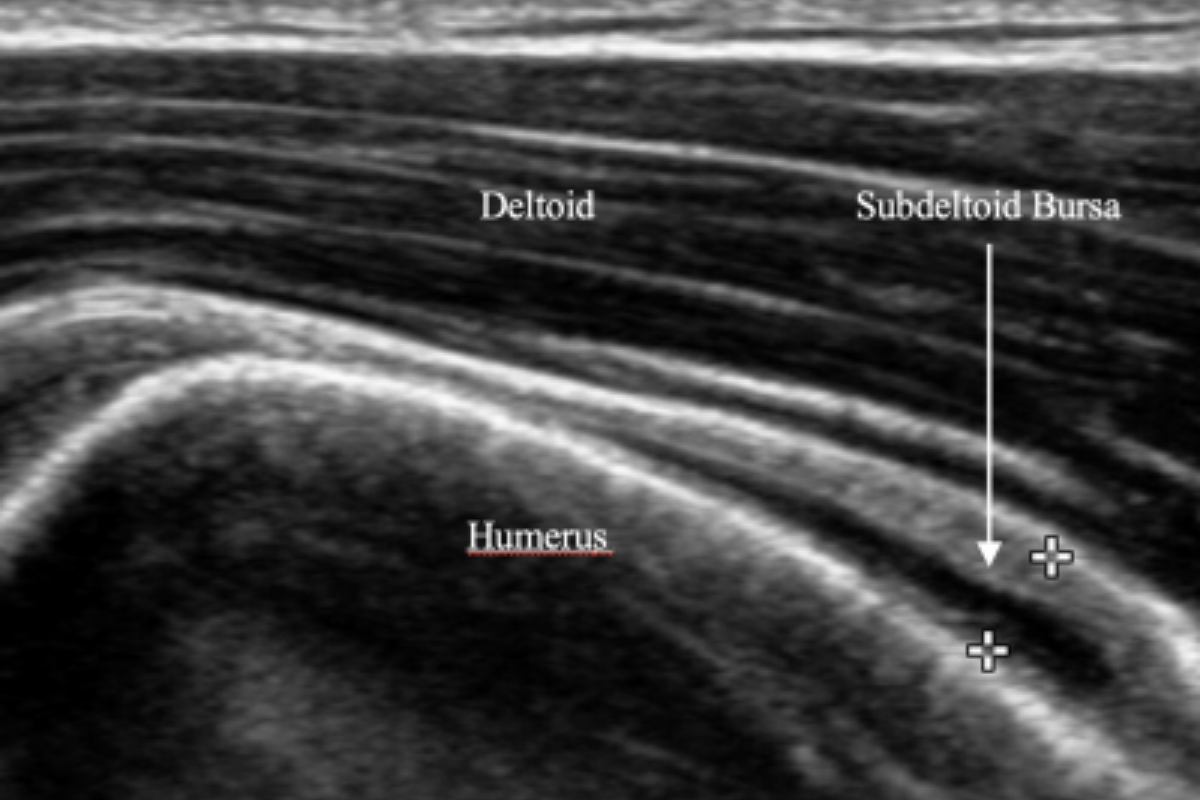
Perhaps on a population level it matters, given that 5% prevalence1 number previously mentioned, suggesting that 5 of 100 shoulder patients we see has isolated teres minor atrophy at a given point in time. But what about at the level of the individual; for the patient presented in this case, did it matter? You will recall that there were other findings in addition to the teres minor atrophy:
The examination indicated: "Subdeltoid/subacromial bursal fluid may indicate bursitis. Teres minor muscle atrophy. Supraspinatus and subscapularis tendons bilateral mild tendinopathy, likely within the normal range for a competitive swimmer.
It seems reasonable to surmise that if there is a decrease in control of the humerus1 as may be predisposed by an atrophied teres minor, then structural changes or injury may result. Of course you may argue, and we would agree, that in order to be competitive at high level swimming, our patient must have been able to compensate adequately for such a loss of movement control of her humerus, especially given that the function of teres minor, lateral rotation of the arm, is shared by infraspinatus.
In summary, we may be a little closer to answering the question of what causes teres minor to atrophy when it has an intact tendon. We may not be any closer to understanding if it matters, and if so, why and how. We have however asked the question, and having asked it lets allow ourselves to continue to be curious.
Keep sending your shoulder cases, and let us know how you go with rehabilitation, especially in cases of isolated teres minor atrophy. With 5 in every 100 cases, between us it shouldn’t take long to begin to see how it matters.
Related reading: shoulder
In the second part of this two part post, learn why indicators of intra-articular pathology seen on ultrasound may require further investigation.