
The ankle 3: consider the foot?
Ankle or foot? Consider both
An 18-year-old man presented having injured his left ankle approximately four days earlier. He required a wheelchair for two days, and was using crutches after that. In addition to obvious pain on weightbearing, he also had bruising apparent in the anterior left leg. Ultrasound examination (Philips iU22, L12-5 MHz and 15-7 MHz Hockey Stick transducers) of the left ankle and foot were performed. The examination suggested a normal ankle examination, with bifurcate calcaneocuboid ligament tear likely complete (Grade 3) and calcaneonavicular ligament partial tear (Grade 2). EDB muscle tear, DTNL partial tear (Grade 2), Gruberis bursitis, and interosseous ligament injury found in the foot.
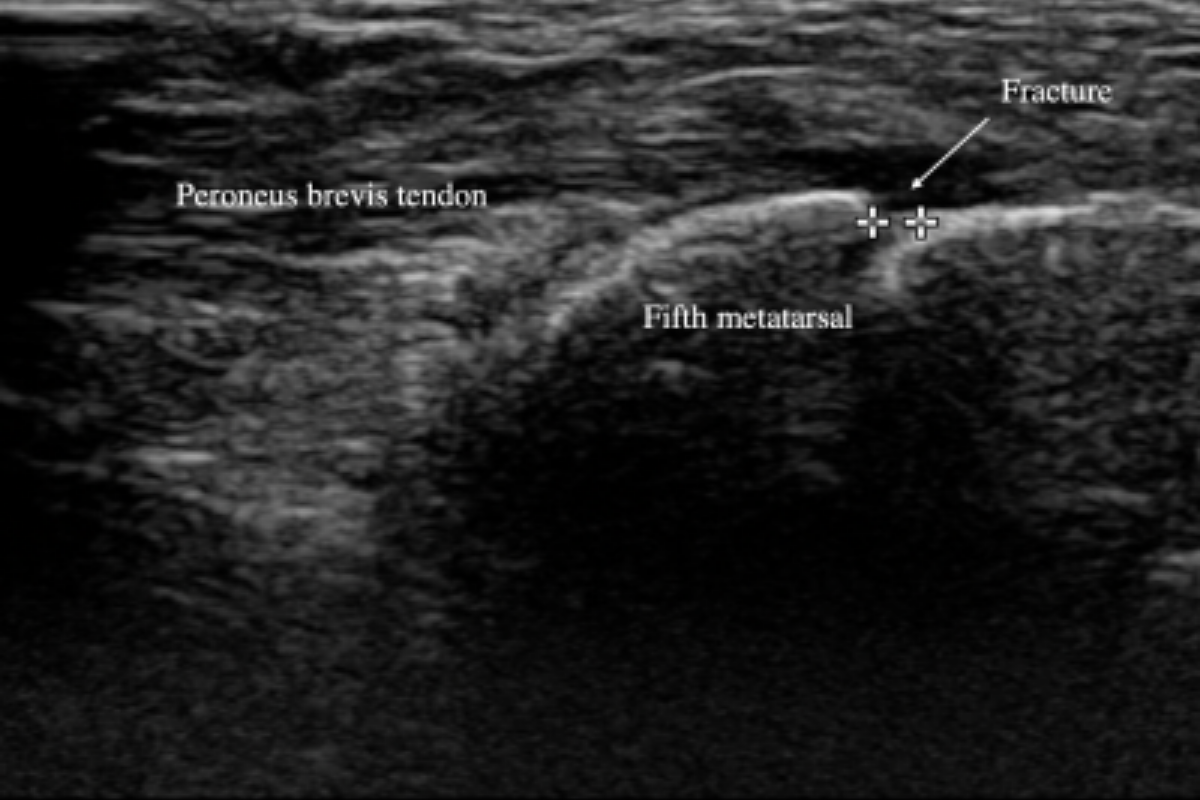
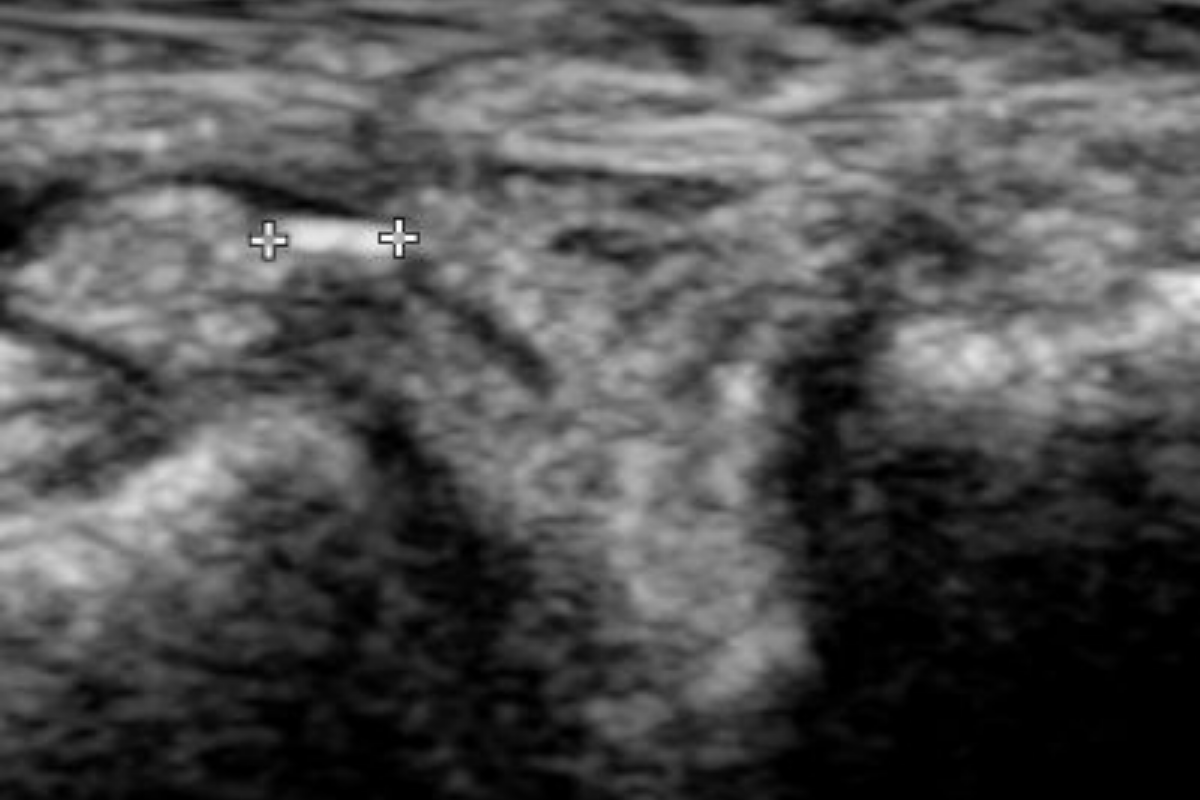
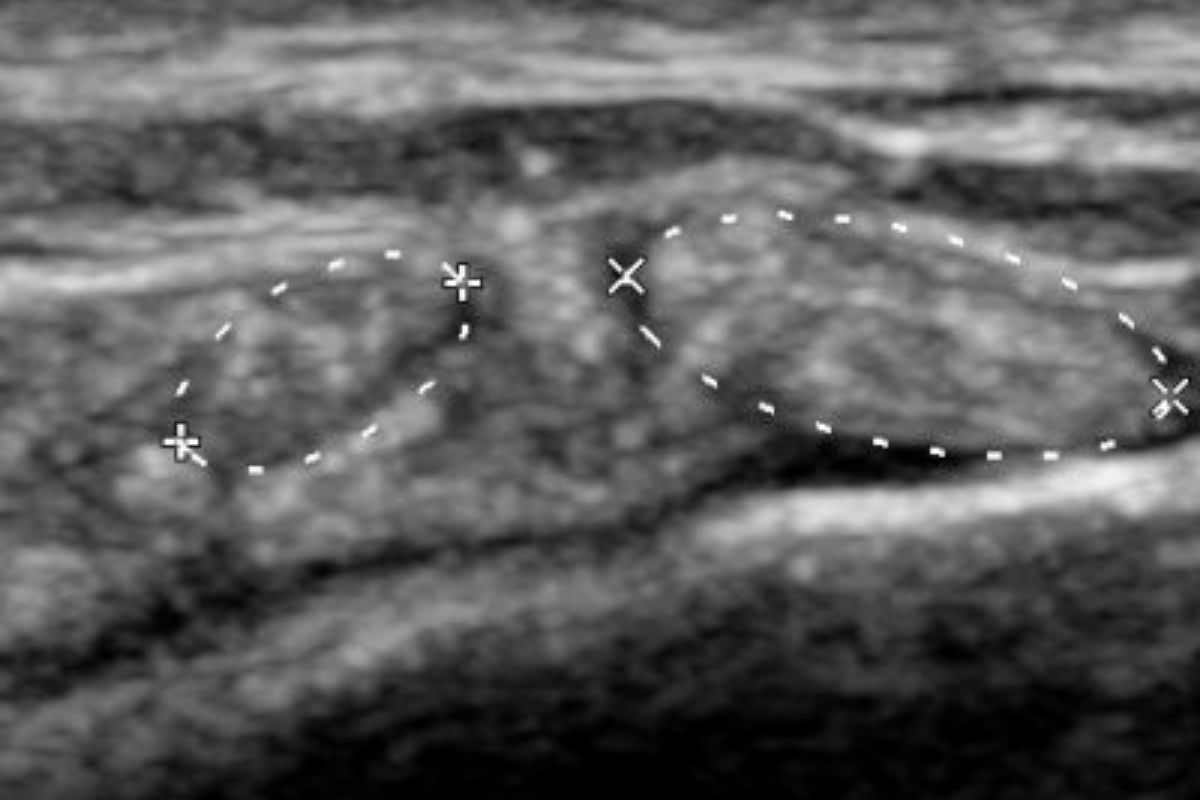
Key findings (Figures A, B, C) included: the calcaneocuboid bifurcate ligament was not identified, there was increased echogenic soft tissue thickening, and a small calcification (2 x 1 mm). The calcaneonavicular bifurcate ligament was thickened and showed reduced echogenicity. The dorsal talonavicular ligament (DTNL) was thick (6 mm), had reduced echogenicity, and had an intrasubstance tear (11 x 6 mm).
When reassessed approximately three months later, the comparison with the previous ultrasound images showed good evidence of healing.
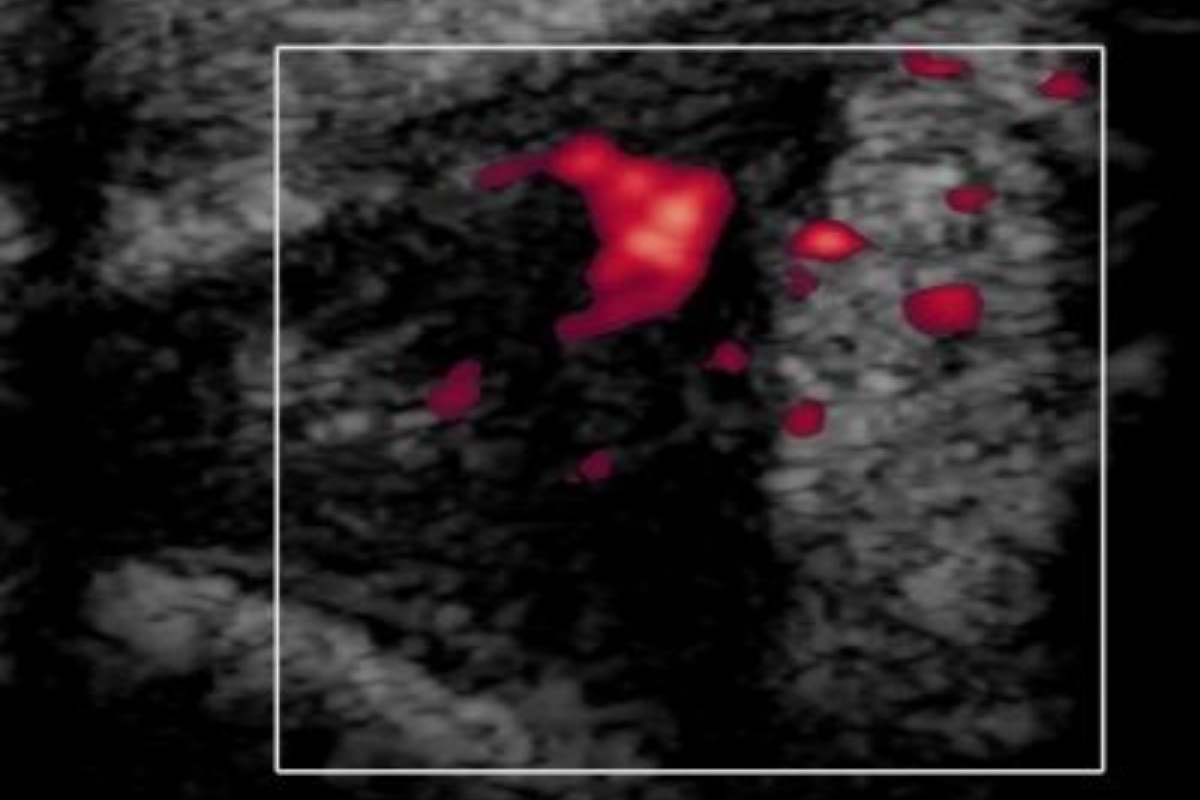
Key findings (Figures D and E) included: the calcaneocuboid joint capsule was mildly thickened. No fluid or vascularity. The bifurcate calcaneonavicular ligament (not shown) was thickened. The dorsal talonavicular ligament was less thickened (5 mm), had reduced echogenicity, and had microcystic change. No vascularity or tear was identified.
Figure A: the calcaneocuboid joint, bifurcate ligament absent, with thickened soft tissue and small calcification
Figure D: the healing calcaneocuboid joint region, remaining soft tissue thickening.
Figure B: the thickened calcaneonavicular bifurcate ligament, indicated by hashmarks.
Figure E: the healing DTNL, remaining thickening, no intrasubstance tear.
Figure C: the thickened DTNL with intrasubstance tear indicated by hashmarks.
The apparent indication for referral in this case was the clinical picture of an ankle injury. It seems probable that the patient had a case history and or clinical presentation suggestive of an ankle sprain, and yet none of the findings were in the region of the ankle. Here again, we think that early and accurate diagnosis can form the basis of the therapeutic reasoning process.
The concept of regional interdependence suggests that musculoskeletal symptoms in one region or joint in the body may be influenced by other body regions and systems1. Certainly when considering the ankle, it makes intuitive sense to consider its association with the adjacent foot. It is not surprising therefore that movements in one are thought to induce movements in the other; the ankle and foot appear to be interdependent2. It may be helpful to consider injury to the foot as a differential diagnosis to be excluded in cases suggestive of ankle injury.
A final point to make here is that while functional assessment of the foot may appear complex3 the improvement seen in the follow-up scan seen in this case demonstrates that management of injuries in the foot follows the same rational management planning4 as elsewhere, and we would contend that a clear diagnosis is likely to facilitate this planning.
References:
Sueki DG, Cleland JA, Wainner RS. A regional interdependence model of musculoskeletal dysfunction: research, mechanisms, and clinical implications. J Man Manip Ther. 2013 May;21(2):90–102.
Ghanem I, Massaad A, Assi A, Rizkallah M, Bizdikian AJ, El Abiad R, et al. Understanding the foot’s functional anatomy in physiological and pathologicalconditions: the calcaneopedal unit concept. J Child Orthop. 2019 Apr;13(2):134–46.
Jarvis HL, Nester CJ, Bowden PD, Jones RK. Challenging the foundations of the clinical model of foot function: further evidencethat the root model assessments fail to appropriately classify foot function. J Foot Ankle Res. 2017;10:7.
English E. Fractures and soft tissue injuries of the feet and ankle. Can Fam Physician. 1985 Mar;31:585–90.
Related reading: ankle

A 60-year-old man presented with left ankle pain after rolling his left ankle. His ankle was extensively bruised and swollen. We explored the injury with ultrasound and X-ray and diagnosed spiral fibula fracture. Urgent surgery was required.